
Adults Tongue Tie Symptoms and Treatment
Most people think tongue tie is a baby problem. Parents hear about it when a newborn struggles to breastfeed, a doctor examines the infant’s mouth, and the simple procedure to release the restriction is performed within days of birth. The story is supposed to end there. But for a significant number of people, tongue tie was never diagnosed in childhood — and they grow up carrying a hidden restriction in their mouth that quietly affects their daily life in ways they never connect to a single physical structure beneath their tongue.
Adult tongue tie is more common than most people realize, and it is considerably more complicated than the infant version. When tongue tie goes untreated into adulthood, the body finds ways to compensate. Other muscles take over functions the tongue should be performing. Posture shifts. Breathing changes. Speech patterns adapt. These compensations can persist even after treatment, which is why adult tongue tie requires a more comprehensive approach than simply snipping a piece of tissue.
If you are an adult who has been told you might have tongue tie, or if you have been living with unexplained symptoms involving speech, swallowing, jaw pain, neck tension, or sleep difficulties, this article gives you a thorough understanding of what adult tongue tie actually is, how it shows up in the body, and what treatment involves.
What Tongue Tie Actually Is in Adults
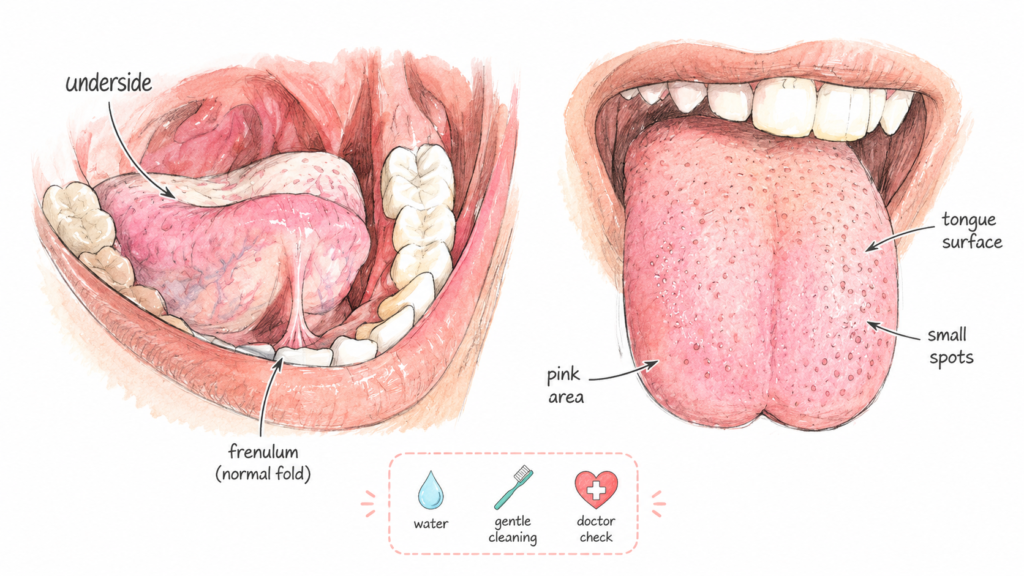
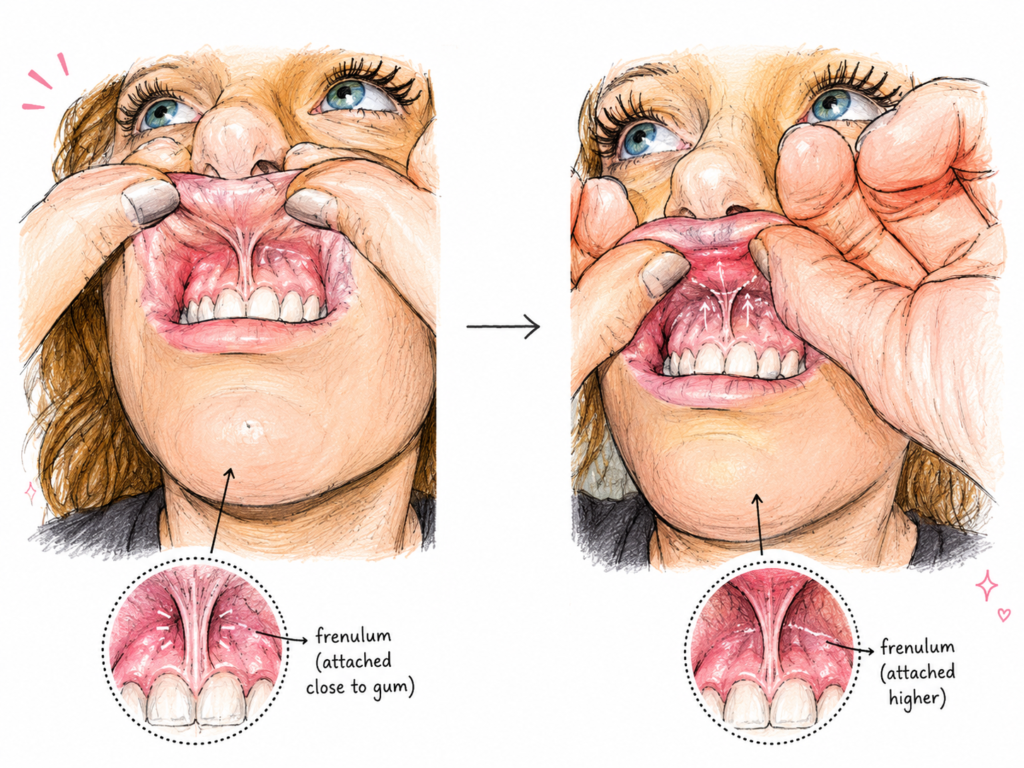
Tongue tie — medically called ankyloglossia — is a condition where the frenulum, the band of tissue that connects the underside of the tongue to the floor of the mouth, is too short, too thick, too tight, or too far forward. This restricts the tongue’s range of motion.
In a normal anatomy, the tongue is highly mobile. It can lift to the roof of the mouth, move freely from side to side, extend past the lips, cup and groove for swallowing, and rest comfortably on the palate. All of these movements are important for breathing, speaking, eating, swallowing, and maintaining proper oral posture.
When the frenulum is restrictive, the tongue cannot perform these movements fully. The degree of restriction varies considerably from person to person. Some people have a very obvious tongue tie where the frenulum is clearly visible and visibly short, pulling the tip of the tongue downward into a heart shape when it tries to lift. Others have what is called a posterior tongue tie — a submucosal restriction that is not easily visible but is felt beneath the mucous membrane and significantly limits tongue elevation and movement.
Adults with tongue tie have been living with this restriction their entire lives. Their brains and bodies have developed enormous compensatory strategies — often completely unconsciously — to manage basic functions like speaking and swallowing despite the limitation. These compensations are what generate many of the symptoms of adult tongue tie, and they are also what makes treatment more involved than in infants.
Classification of tongue tie by severity:
| Classification | Description | Visible to Naked Eye? | Typical Restriction Level |
|---|---|---|---|
| Class 1 (Anterior) | Frenulum attaches near tongue tip | Yes, clearly | Severe movement restriction |
| Class 2 (Anterior) | Frenulum attaches slightly further back | Yes | Moderate to severe |
| Class 3 (Posterior) | Frenulum under mucosa, mid-tongue | Not easily | Moderate |
| Class 4 (Posterior) | Deep submucosal, rear of tongue | Not visible | Mild to moderate, often missed |
Why So Many Adults with Tongue Tie Were Never Diagnosed
A natural question is: how does someone go through childhood, teenage years, and into adulthood with a tongue tie and never be told about it? The answer involves a combination of historical diagnostic gaps, inconsistent clinical training, and the remarkable adaptability of the human body.
Before the current wave of interest in tongue tie — which has grown significantly in the past 15 to 20 years largely driven by lactation consultants and a more comprehensive understanding of oral function — many healthcare providers had minimal training in identifying tongue tie beyond the most obvious anterior cases. A posterior tongue tie that lies hidden under the mucosa requires deliberate examination with a gloved finger to palpate the restriction. Most routine physical examinations in children and adults do not include this check.
The human body is also extraordinarily good at compensating for physical limitations. A child who cannot lift their tongue properly learns to speak by recruiting other articulators — the lips, cheeks, jaw — to help produce sounds that would normally require tongue elevation. A person who cannot swallow normally because their tongue cannot cup food effectively learns to tilt the head, thrust the jaw, or use more forceful swallowing patterns. These compensations work well enough that the person functions in daily life without obvious disability. The underlying restriction is there, but the symptoms it produces seem unrelated to the mouth.
Another factor is that symptoms of tongue tie in adults are often attributed to other causes. Jaw pain gets diagnosed as temporomandibular joint disorder. Neck tension is attributed to posture or stress. Speech difficulty is assumed to be a speech impediment unrelated to anatomy. Sleep apnea is treated without examining whether tongue posture is a contributing factor. Each symptom is managed in isolation without anyone connecting the dots back to a short frenulum.
Reasons adult tongue tie is frequently missed:
- Posterior tongue tie is not visible without active palpation
- Medical training historically focused only on obvious anterior tongue ties
- Compensatory adaptations make function appear adequate on casual examination
- Symptoms are typically attributed to other conditions
- Adults rarely have routine oral function assessments
- Short frenum may not appear significant unless tongue range of motion is specifically tested
- No standard screening protocol for tongue tie in adult medical examinations
The Tongue’s Role in the Body That Most People Never Think About
To understand why a restricted tongue creates such wide-ranging symptoms in adults, it helps to understand everything the tongue is supposed to do. Most people think of the tongue primarily in terms of speech and taste. The reality is much broader.
The tongue is a powerful muscle — actually a group of eight muscles — that plays a central role in oral function from the moment of birth. In infancy, the tongue creates suction during breastfeeding. Later it moves food during chewing, guides the food bolus to the back of the mouth, and initiates the swallowing reflex. It generates the pressure changes needed for the Eustachian tubes to function properly, affecting ear health and middle ear pressure. It helps develop the shape of the dental arch and palate through the pressure of resting contact — a tongue that rests properly on the roof of the mouth provides constant gentle force that shapes the upper jaw from inside. It plays a critical role in breathing by positioning the airway during sleep. And it is involved in head and neck posture through its fascial connections down through the floor of the mouth, the throat, and even the hyoid bone.
When the tongue is restricted, none of these functions work as well as they should. The developmental consequences in childhood include narrow dental arches, crowded teeth, high-arched palates, and increased risk of mouth breathing. In adulthood, the functional consequences include everything from swallowing difficulties to jaw disorders to neck pain to sleep-disordered breathing.
Functions of the tongue affected by restriction:
| Tongue Function | Effect When Restricted | Resulting Symptom |
|---|---|---|
| Suction and swallowing | Compensatory swallowing patterns | Choking, difficulty with certain foods |
| Palate development | Narrow arch, high palate | Crowded teeth, nasal congestion |
| Dental arch pressure | Reduced expansion force | Crossbite, narrow jaw |
| Airway positioning during sleep | Low tongue posture | Snoring, sleep apnea |
| Speech production | Cannot reach palate for sounds | Articulation difficulties |
| Head and neck posture | Altered fascial tension | Neck pain, headaches |
| Eustachian tube function | Insufficient pressure equalization | Ear popping, fullness, fluid |
Speech Symptoms That Tongue Tie Creates in Adults
Speech is one of the most immediately affected functions in many adults with tongue tie. The sounds most commonly affected are those that require the tongue tip or tongue body to lift to the palate or the tooth ridge behind the front teeth.
The sounds typically affected include T, D, N, L, R, S, Z, and combinations of these sounds. In severe anterior tongue tie, these sounds may be noticeably slurred, substituted, or omitted. More commonly in adults who have had years of compensatory practice, the sounds may be produced in a way that sounds close enough to normal that no one identifies a speech problem — but the person works harder than necessary to produce them, experiences fatigue during extended speaking, or notices that certain sounds feel effortful.
Many adults with tongue tie report that they speak faster or more quietly than they would like to, not from personality but because extended speech is physically tiring. Public speaking may feel exhausting in a way that seems out of proportion to the situation. Some people notice that their speech becomes less clear when they are tired, because the compensatory strategies that cover for the restricted tongue require mental and muscular effort that diminishes with fatigue.
Lisping is one of the more recognizable speech patterns associated with tongue tie in adults. Both the classic frontal lisp (where S sounds more like TH) and the lateral lisp (where air escapes around the sides of the tongue during S sounds) can be related to restricted tongue elevation and tongue tip mobility.
Dr. Robyn Merkel-Walsh, a licensed speech-language pathologist and a leading expert in oral motor function, has written that many adults who have received speech therapy for years without achieving normal articulation for certain sounds may have an undiagnosed tongue tie. The therapy teaches compensatory movements but cannot overcome a mechanical restriction that prevents the target movement.
Speech sounds commonly affected by adult tongue tie:
| Sound | Normal Tongue Position Required | How Restriction Affects It |
|---|---|---|
| T and D | Tongue tip touches tooth ridge | Imprecise contact, muffled quality |
| L | Tongue tip lifts to palate | Reduced clarity, substitution |
| R | Tongue body bunches or tip curls | Distorted R, common area of difficulty |
| S and Z | Narrow tongue groove | Frontal or lateral lisp |
| N | Tongue tip to tooth ridge with nasal airflow | Reduced clarity |
| TH | Tongue tip between teeth or at edge | Variable, sometimes less affected |
| Hard G and K | Back of tongue raises to soft palate | Generally less affected |
Swallowing Patterns and Their Connection to Tongue Restriction
Swallowing is something adults do around 2,000 times every day without thinking about it. Most people swallow without any awareness unless something goes wrong. When the tongue is restricted, swallowing works differently — and the patterns that develop to compensate for the restriction can cause problems over time.
Normal swallowing involves the tongue rising to the roof of the mouth, cupping the food or liquid, and pushing it backward in a coordinated wave that initiates the swallow reflex. The teeth come together lightly, the tongue presses to the palate, and the throat muscles coordinate the passage of food downward while the airway is briefly protected.
In adults with tongue tie, the tongue often cannot rise fully to the palate. Instead, several compensatory swallowing patterns develop. Tongue thrusting — where the tongue pushes forward against or between the teeth during the swallow rather than rising upward — is one of the most common. This creates forward pressure on the front teeth, contributing to gaps between the upper front teeth or an open bite. It can also contribute to dental relapse after orthodontic treatment, frustrating patients and orthodontists alike.
Other compensatory swallowing patterns include using the cheeks and facial muscles excessively during swallowing, tilting the head forward or backward to use gravity to assist the swallow, and using a high-volume, forceful swallow to compensate for poor tongue coordination.
These compensatory patterns place abnormal forces on the teeth, jaw joints, and surrounding muscles. Over years and decades, they contribute to the jaw pain, facial tension, and dental problems that many adults with undiagnosed tongue tie experience.
Swallowing compensation patterns in adults with tongue tie:
- Tongue thrusting forward against or between front teeth during swallows
- Excessive facial and cheek muscle contraction during swallowing
- Tilting the head to assist food movement
- Swallowing with excessive force or multiple swallows per bolus
- Difficulty swallowing pills or large food pieces
- Sensation of food getting stuck in the throat
- Needing to drink water frequently while eating to help food go down
- Preference for softer foods that require less tongue manipulation
Jaw, Neck, and Head Pain Linked to Compensatory Muscle Use
The muscles of the jaw, neck, and head work in close coordination with the tongue through fascial connections and shared functional roles. When the tongue is restricted and cannot perform its natural functions, other muscles compensate. They perform work they were not designed to do, repeatedly, day after day, for years or decades. The result is chronic overuse, tension, and pain in these muscle groups.
The temporomandibular joint (TMJ) and the muscles that control jaw movement are commonly affected. Many adults with undiagnosed tongue tie carry a diagnosis of temporomandibular joint disorder (TMD) — characterized by jaw clicking, popping, limited mouth opening, jaw pain, and facial pain. The connection to tongue tie is that when the tongue cannot rest properly on the palate and cannot coordinate swallowing normally, the jaw must compensate during swallowing and chewing, creating abnormal strain on the TMJ over time.
The suprahyoid muscles — the group of muscles above the hyoid bone in the throat — are directly attached to the floor of the mouth and the tongue. In tongue tie, these muscles are often under chronic tension because they are constantly working to help the restricted tongue perform functions it cannot achieve on its own. This chronic tension radiates upward into the jaw, the floor of the mouth, the cheeks, and the temples, contributing to facial pain, headaches, and jaw tightness.
The neck and shoulder muscles also become involved through postural adaptation. When the tongue rests low in the mouth rather than on the palate — because elevation is restricted — the head tends to shift forward on the spine to compensate for the change in airway space and balance. Forward head posture places chronic strain on the neck extensor muscles, contributing to the neck pain, stiffness, and headaches that many adults with tongue tie report.
Muscle and joint symptoms associated with adult tongue tie:
| Area | Common Symptoms | Connection to Tongue Restriction |
|---|---|---|
| TMJ (jaw joint) | Clicking, pain, limited opening | Abnormal jaw loading during compensatory swallowing |
| Masseter muscles | Jaw clenching, facial soreness | Overuse compensation for tongue restriction |
| Suprahyoid muscles | Floor of mouth tension, throat tightness | Direct attachment to tongue and floor of mouth |
| Neck extensors | Neck pain, stiffness, tension headaches | Forward head posture from low tongue resting position |
| Temporal muscles | Temple headaches, tension | Continuous jaw and facial muscle compensation |
| Shoulder muscles | Upper shoulder tension | Postural chain effects of forward head posture |
Sleep Problems Adults Tongue Tie Symptoms
One of the most significant and increasingly discussed connections in adult tongue tie is the relationship between restricted tongue function and sleep-disordered breathing, including obstructive sleep apnea and upper airway resistance syndrome.
During sleep, the body’s muscles relax. The tongue, being a muscular structure, also relaxes. When the tongue is resting in its proper position — against the roof of the mouth (the palate) — it supports the airway space during sleep. When the tongue cannot reach the palate due to restricted elevation, it falls back toward the floor of the mouth and potentially toward the back of the throat, reducing the airway space and increasing the likelihood of airway obstruction during sleep.
Research examining the anatomy of people with obstructive sleep apnea has found that low tongue posture is significantly associated with airway collapsibility. Dr. Christian Guilleminault, a pioneering sleep medicine researcher at Stanford University, published extensively on the connection between restricted oral development, low tongue posture, and sleep-disordered breathing. His research pointed to tongue tie and myofunctional disorders as upstream factors in many cases of obstructive sleep apnea, particularly in children and young adults.
Adults with tongue tie who have sleep apnea may find that their sleep apnea is not fully resolved by CPAP therapy alone if the underlying tongue posture and oral function are not also addressed. Myofunctional therapy to improve tongue posture and strength, in conjunction with treatment for the tongue tie, can provide more comprehensive and lasting improvement in airway function during sleep.
Snoring, morning headaches, waking unrefreshed, dry mouth upon waking (indicating mouth breathing during sleep), and excessive daytime sleepiness are all symptoms that adults with tongue tie should pay attention to and discuss with both their dentist or oral health specialist and their physician.
Sleep and breathing symptoms in adults with tongue tie:
- Chronic snoring
- Obstructive sleep apnea or symptoms consistent with it
- Waking with a dry mouth (sign of mouth breathing during sleep)
- Mouth breathing during sleep and waking hours
- Unrefreshed sleep despite adequate duration
- Morning headaches
- Daytime fatigue and difficulty concentrating
- Upper airway resistance syndrome
Dental Problems That Frequently Accompany Adult Tongue Tie
The teeth and the jaws develop in response to the forces placed upon them throughout childhood. The tongue provides outward pressure on the dental arch from inside, helping to shape a wide, well-developed arch. Lips and cheeks provide inward pressure from outside. When these forces are balanced, the result is a well-shaped jaw with room for all the teeth.
When tongue tie prevents normal tongue posture and function in childhood, the inward forces from the lips and cheeks dominate without adequate outward counter-pressure from the tongue. The result is often a narrowed upper arch, high palate, and crowded teeth. Many adults with tongue tie had braces or orthodontic treatment to correct crowding that was actually downstream of the tongue restriction — and without addressing the restriction, some experience orthodontic relapse, with teeth shifting back toward their original positions over time.
Open bite — where the front teeth do not touch even when the back teeth are closed — is associated with tongue thrusting during swallowing, itself a compensation for tongue restriction. Cross bite, where the upper teeth sit inside the lower teeth on one or both sides, is associated with the narrow upper arch that develops when the tongue cannot provide normal outward pressure.
Excessive tooth wear can occur in areas where the tongue is pressing unusually hard during compensatory swallowing. Gum recession in the lower front teeth is sometimes seen in people whose tongue is chronically pressing against those teeth.
Dental and orthodontic issues associated with adult tongue tie:
| Dental Problem | Connection to Tongue Restriction | How It Develops |
|---|---|---|
| Crowded teeth | Narrow arch from insufficient tongue outward pressure | Tongue cannot provide arch expansion during growth |
| High-arched palate | Tongue resting low, not on palate | Palate shaped by lack of tongue contact |
| Open bite | Tongue thrusting during swallowing | Constant forward tongue pressure on front teeth |
| Cross bite | Narrow upper arch | Imbalanced pressure forces on developing jaw |
| Diastema (gap between front teeth) | Tongue thrust or low tongue rest | Tongue pressure pushes front teeth apart |
| Orthodontic relapse | Uncorrected swallowing pattern continues | Tongue forces undo orthodontic correction |
Digestive and Eating Difficulties That Adults Often Overlook
Many adults with tongue tie have eating habits and preferences that they consider personal quirks but are actually adaptations to restricted tongue function. The connection is rarely made until someone examines their oral function specifically.
Difficulty chewing tough or chewy foods — steak, raw carrots, crusty bread, chewy candies — is common. The tongue is supposed to manipulate food during chewing, moving it from side to side across the molars and repositioning it for efficient breakdown. When the tongue is restricted, this manipulation is labored. The person may avoid tough foods, cut everything very small, swallow food less thoroughly chewed than ideal, or take significantly longer to eat a meal than their dining companions.
Gagging easily is a frequent complaint. When the tongue cannot coordinate the passage of food properly, the swallowing reflex may be triggered at an unusual time or in an unusual way, creating a gag response. Some adults with tongue tie report having strong gag reflexes that make dental procedures particularly difficult.
Digestive symptoms like bloating, gas, and indigestion can sometimes be connected to swallowing patterns. When food is not chewed thoroughly because tongue manipulation is limited, larger food particles reach the stomach. When air is swallowed in greater amounts due to compensatory swallowing movements, gas and bloating can result. These are not absolute or universal symptoms, but they are reported often enough in tongue tie communities to be worth noting.
Eating and digestive symptoms in adults with tongue tie:
- Difficulty with tough, chewy, or crunchy foods
- Eating very slowly compared to others
- Needing to drink frequently while eating
- Swallowing food in larger pieces than ideal
- Strong gag reflex, especially at the dentist or during certain foods
- Difficulty eating without making noise (related to compensatory tongue movements)
- Bloating or gas after meals
- Preference for soft foods
- Difficulty managing thin liquids without coughing or choking
Emotional and Psychological Effects of Living with Untreated Tongue Tie
The physical symptoms of tongue tie are well-established, but the psychological and social impacts are less often discussed and deserve attention. Adults who have spent a lifetime compensating for a restricted tongue often carry invisible emotional burdens related to their speech, eating, and social interactions.
Speech difficulties — even subtle ones — can create significant self-consciousness. Adults who slur certain sounds, speak less clearly when tired, or feel their speech sounds different from everyone around them may avoid speaking in public, shy away from presentations, or feel anxious in social situations involving speaking. Because the cause is physical, speech therapy may have had limited success, leaving the person feeling frustrated and as though the difficulty is a personal failing rather than a mechanical restriction.
Eating in social situations can also be a source of anxiety. Adults who eat slowly, make noises while eating, or need to manage food in specific ways to compensate for tongue restriction may feel embarrassed at meals. They may avoid certain restaurants, decline invitations where eating in public is involved, or feel self-conscious when dining with new people.
The persistent fatigue of sleep apnea connected to tongue tie affects mood, energy, relationships, and professional functioning. Chronic headaches and jaw pain affect quality of life in ways that are difficult to quantify but very real.
When adults finally receive a tongue tie diagnosis after years of unexplained symptoms, the most common response — according to clinical reports from practitioners in this field — is a combination of relief and frustration. Relief that there is a name and a reason for what they have experienced. Frustration that it was not identified sooner.
Psychological and social impacts of adult tongue tie:
- Speech-related anxiety and avoidance of speaking situations
- Self-consciousness about eating in public
- Frustration from speech therapy that did not achieve full improvement
- Difficulty understanding why certain efforts produce limited results
- Fatigue and mood effects from poor sleep quality
- Reduced professional confidence when speaking is involved
- Relief at diagnosis combined with frustration about years without identification
How Adult Tongue Tie Is Diagnosed
Diagnosing tongue tie in adults requires a thorough clinical assessment by a provider who understands the full functional picture, not just the visible anatomy. The most qualified providers for this assessment include dentists or oral surgeons who specialize in tongue tie, myofunctional therapists, speech-language pathologists with specific training in orofacial myology, and in some cases ENT specialists.
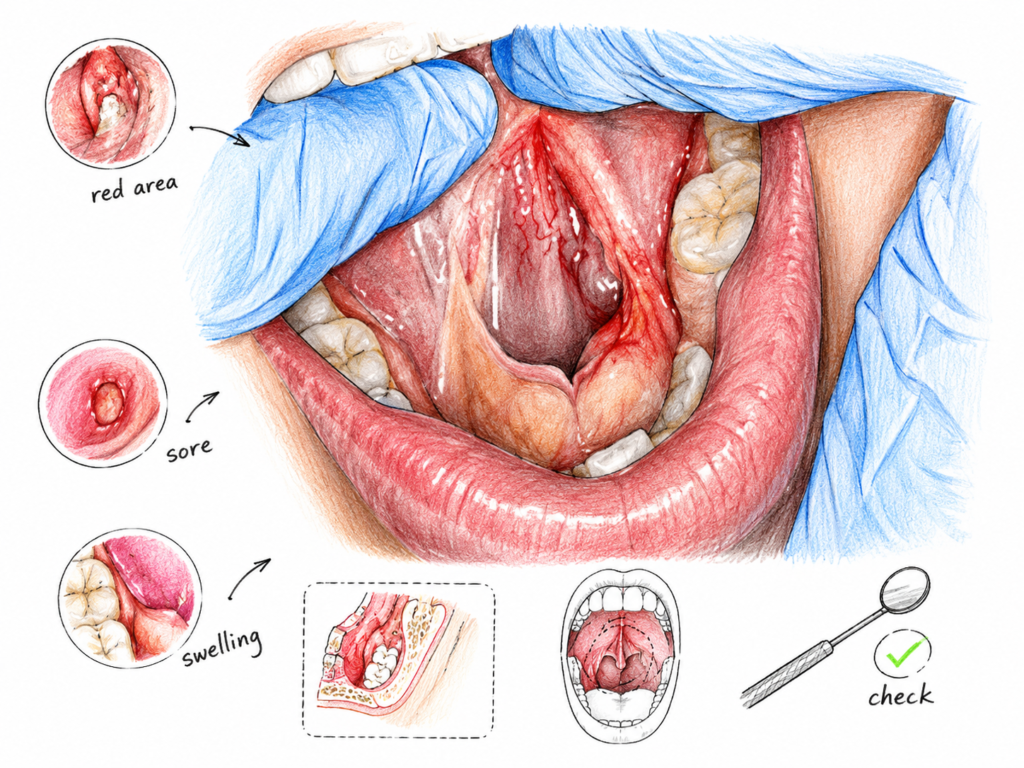
The assessment includes a visual examination of the frenulum to look for obvious anterior attachment, but it must also include palpation — using a gloved finger to lift the tongue and feel for a submucosal restriction beneath the mucous membrane. Many posterior tongue ties are invisible to visual inspection and only detectable by palpation.
The functional examination is equally important. The clinician asks the patient to perform specific tongue movements: lift the tongue to the palate with the mouth open, sweep the tongue around the inside of the lips, stick the tongue out as far as possible, move it from side to side, and attempt to touch the tip of the tongue to the nose and chin. Limitations in any of these movements, combined with the patient’s symptom history, help confirm the diagnosis.
The Kotlow classification system and the Hazelbaker Assessment Tool are among the commonly used clinical tools for grading tongue tie severity. More recently, several researchers and clinicians have developed comprehensive assessment protocols that incorporate functional measures beyond just the appearance of the frenulum.
Imaging such as ultrasound can be used in research settings to visualize tongue movement, and some specialized clinics use this for assessment. However, a thorough clinical examination by an experienced provider remains the standard diagnostic approach.
What a tongue tie assessment for adults includes:
- Full medical and symptom history — asking about speech, sleep, swallowing, jaw pain, and dental history
- Visual inspection of the frenulum — looking for short, tight, or anteriorly placed attachment
- Palpation of the floor of the mouth — feeling for submucosal restriction
- Tongue movement testing — lifting, sweeping, protrusion, lateral movement
- Oral posture assessment — where the tongue rests at rest and during swallowing
- Speech screening — listening for patterns consistent with restricted tongue movement
- Dental examination — looking for arch shape, palate height, bite pattern, and wear patterns
- Referral to myofunctional therapist, speech therapist, or other specialists as appropriate
Treatment for Adult Tongue Tie — The Full Picture
Treating adult tongue tie is a multi-step process that involves more than just the release procedure. Understanding the full treatment framework helps adults set realistic expectations and achieve the best possible outcomes.
Pre-treatment myofunctional therapy
Before any release procedure is performed on an adult, most experienced practitioners recommend a course of myofunctional therapy — typically 4 to 8 weeks. This involves exercises designed to improve tongue strength, range of motion, and awareness. The rationale is practical: an adult with tongue tie has spent years using compensatory muscle patterns. If the restriction is released without first beginning to retrain these patterns, the compensations continue. The muscles that were overworked remain overworked. The brain does not automatically know how to use the tongue differently. Pre-treatment therapy also helps the patient understand what normal tongue function feels like and gives them a baseline for noticing improvement after the release.
The release procedure (Frenectomy or Frenotomy)
The release procedure involves cutting or removing the restrictive frenulum tissue to allow greater tongue mobility. In adults, two main approaches are used.
A scalpel frenectomy is performed by an oral surgeon or dentist under local anesthesia. The frenulum is cut with a surgical blade and the wound is typically sutured. This approach is precise and allows complete removal of the frenulum tissue. Recovery involves some soreness and dietary modification for several days.
Laser frenectomy uses a soft tissue laser (typically a CO2 or diode laser) to remove the frenulum tissue. Laser procedures have the advantage of minimal bleeding during the procedure, reduced bacterial contamination risk, and often faster initial healing. Some practitioners prefer laser for the precision it allows, particularly when dealing with posterior tongue ties. Recovery is generally similar to scalpel procedures.
The choice between scalpel and laser depends on the specific anatomy, the practitioner’s preference and training, and the location and type of tongue tie.
Post-treatment stretching and exercises
After the release, the healing tissue has a strong tendency to reattach. The mouth heals quickly, and scar tissue can form across the release site if it is not actively prevented. For this reason, post-operative exercises — called wound stretches — are essential in the days and weeks following the procedure. These involve gently lifting the tongue and pressing on the diamond-shaped wound site to prevent the edges from adhering together.
Post-release myofunctional therapy continues and intensifies after the procedure. The tongue now has physical freedom it did not have before, but the brain and muscles still have their old patterns. Therapy helps reprogram the tongue’s function — teaching it to rest on the palate, coordinate normal swallowing, and use its full range of motion in speech.
Timeline of adult tongue tie treatment:
| Phase | What Happens | Duration |
|---|---|---|
| Initial assessment | Diagnosis, functional evaluation, referral | 1 to 3 appointments |
| Pre-operative myofunctional therapy | Exercises to prepare muscles and establish awareness | 4 to 8 weeks |
| Release procedure | Frenectomy under local anesthesia | Single appointment |
| Immediate post-operative care | Wound stretches, soft diet, pain management | 2 to 4 weeks |
| Post-operative myofunctional therapy | Retraining tongue function, reprogramming swallowing | 3 to 6 months |
| Speech therapy (if needed) | Correcting residual articulation patterns | Variable |
| Review and follow-up | Confirming range of motion and function | Ongoing as needed |
Myofunctional Therapy — What It Is and Why Adults Need It
Myofunctional therapy is a specialized form of therapy that addresses the function of the oral and facial muscles. It is performed by a trained orofacial myofunctional therapist (OMT) — which may be a speech-language pathologist, a dental hygienist, or another healthcare professional who has completed specific training in this area.
The therapy consists of a structured program of exercises targeting the tongue, lips, cheeks, and jaw. For adults being treated for tongue tie, myofunctional therapy is not optional — it is an essential part of achieving meaningful functional improvement. Without it, the release procedure alone often produces disappointing results.
The goals of myofunctional therapy for adult tongue tie include establishing proper tongue resting posture (tongue on the palate, lips closed, breathing through the nose), retraining a normal swallowing pattern without tongue thrust, improving tongue strength and coordination for speech, establishing nasal breathing as the default pattern, and reducing the compensatory muscle tensions in the jaw, neck, and throat.
Therapy typically involves weekly or biweekly sessions with the therapist and daily home exercises. A typical program lasts 4 to 6 months, sometimes longer depending on the complexity of the case and the degree of compensatory patterns that need to be addressed.
The concept of neuroplasticity — the brain’s ability to form new connections and learn new movement patterns — is central to myofunctional therapy. The brain learned the old compensatory patterns over years of practice. It can learn new, functional patterns with consistent, deliberate exercise. Adults often progress somewhat more slowly than children because their compensatory patterns are more deeply established, but meaningful change is entirely achievable at any age.
What myofunctional therapy exercises include:
- Tongue elevation exercises — pressing the tongue to the palate and holding
- Tongue lateralization — moving the tongue side to side with precision
- Tongue tip placement — precisely placing the tongue tip at specific spots on the palate
- Nasal breathing training — exercises and habits to establish nose breathing
- Swallowing retraining — learning to swallow with the tongue on the palate rather than thrusting forward
- Lip strengthening and closure — building lip muscle tone for resting lip seal
- Jaw relaxation exercises — releasing chronic jaw and facial muscle tension
- Cheek and facial muscle exercises — reducing overuse compensation in these muscles
What to Expect in Recovery After a Tongue Tie Release
Adults frequently want to know what recovery from a frenectomy is like. The honest answer is that it is more involved than infant tongue tie release but very manageable with proper preparation and aftercare.
On the day of the procedure, local anesthetic is used, so the procedure itself is not painful. The tongue may feel numb for a few hours afterward. As the anesthetic wears off, soreness in the floor of the mouth begins, typically described as feeling similar to a pulled muscle or the soreness after a dental injection.
Over the following several days, the wound site forms a white or yellowish diamond-shaped area of healing tissue. This is normal and does not indicate infection. Swallowing may be uncomfortable during the first few days. Most adults take over-the-counter pain medication as needed and manage well.
Eating soft foods for the first week to ten days is generally recommended. Avoiding foods that require a lot of tongue movement or that are hot, spicy, acidic, or crunchy reduces irritation to the healing site.
The wound stretching exercises — typically starting 24 to 48 hours after the procedure and continuing for 4 to 6 weeks — are the most challenging part of recovery for many adults. They involve placing a finger under the tongue and gently but firmly lifting and spreading the wound edges to prevent reattachment. These exercises can be uncomfortable, particularly in the first week. Consistency with these exercises is critical to preventing restrictive scar tissue formation.
The tongue may feel strange, heavy, or different after the release. This is because the anatomy has changed and the brain is processing new information from the proprioceptors in the tongue and floor of the mouth. This adjustment period is normal and typically resolves over several weeks as the brain adapts.
Week-by-week recovery overview:
| Week | Physical Experience | Key Actions |
|---|---|---|
| Week 1 | Soreness, numbness, healing wound forms | Soft diet, wound stretches begin, manage pain |
| Week 2 | Soreness decreasing, white area shrinking | Continue stretches, begin post-op therapy |
| Weeks 3 to 4 | Near-normal eating returning, tongue feels different | Continue stretches, active therapy exercises |
| Weeks 5 to 6 | Stretches finishing, tongue mobility increasing | Active myofunctional therapy focus intensifies |
| Month 2 to 3 | New movement patterns developing | Consistent therapy, speech if needed |
| Month 4 to 6 | Functional improvements becoming evident | Continued therapy, reassessment of function |
Finding the Right Healthcare Team for Adult Tongue Tie
One of the practical challenges for adults seeking tongue tie evaluation and treatment is finding providers who have genuine expertise in this area. Not every dentist, oral surgeon, or speech therapist has trained specifically in adult tongue tie assessment and management.
The most effective treatment for adult tongue tie involves a team approach. The core team typically includes a tongue tie specialist (dentist, oral surgeon, or periodontist with specific tongue tie training) who performs the release procedure, and a myofunctional therapist who provides pre- and post-operative therapy. A speech-language pathologist with training in orofacial myology may be involved if articulation goals are part of the treatment plan. In cases involving sleep apnea, a sleep medicine physician may be part of the team. For dental concerns like orthodontic relapse or bite issues, an orthodontist familiar with oral function issues is valuable.
Finding practitioners can take some effort. Professional organizations such as the Academy of Orofacial Myofunctional Therapy (AOMT) and the International Affiliation of Tongue Tie Professionals (IATP) maintain practitioner directories that can help locate qualified providers. Online communities for adults with tongue tie are also a source of practitioner recommendations from people who have personal experience.
When consulting with a potential provider, asking specifically about their training and experience with adult posterior tongue ties is important. A provider who is primarily experienced with infant tongue tie may not have the full assessment and treatment approach needed for adults with years of compensatory patterns.
Questions to ask a potential tongue tie provider:
- Do you assess posterior tongue ties in adults, including palpation?
- How many adult tongue tie procedures do you perform annually?
- Do you require or recommend pre-operative myofunctional therapy?
- Who do you recommend for myofunctional therapy in this area?
- What post-operative stretching protocol do you use?
- How do you follow up after the procedure?
- Do you work with a team including speech therapists and myofunctional therapists?
Managing Expectations — What Tongue Tie Release Can and Cannot Fix
Adults considering tongue tie treatment deserve an honest picture of what treatment can realistically achieve. Treatment can produce genuinely significant improvements in quality of life for many adults — improvements in speech clarity, jaw comfort, sleep quality, swallowing ease, and neck tension are all documented outcomes. But treatment is not a simple fix, and not every symptom attributable to tongue tie will fully resolve.
The degree of improvement depends on how severe the original restriction was, how well the release procedure is performed, how thoroughly the wound heals without reattachment, and — critically — how diligently the patient engages in myofunctional therapy before and after the procedure. Adults who do the pre-operative therapy, follow the post-operative stretching protocol carefully, and commit to months of myofunctional exercises have significantly better outcomes than those who treat the release procedure as an isolated event.
Some compensatory patterns are deeply established enough that they do not fully resolve even with excellent myofunctional therapy. Speech patterns that have been habitual for 30 or 40 years may improve but not reach the same level as someone treated at age 5. Jaw joint damage from decades of abnormal loading may be reduced but not completely reversed. Sleep apnea related to tongue posture may improve but may still require additional management.
Setting realistic expectations — that treatment is a significant positive change that requires effort and time, rather than an instant cure — helps adults approach the process with the patience and commitment that produces the best outcomes.
Realistic outcome expectations for adult tongue tie treatment:
| Symptom Area | Typical Improvement | What May Persist |
|---|---|---|
| Tongue range of motion | Significant improvement | Some limitation may remain with severe posterior ties |
| Speech clarity | Moderate to significant | Long-established habits may need ongoing therapy |
| Swallowing pattern | Good improvement with therapy | Some compensation may persist without consistent exercise |
| Jaw and neck pain | Often significant reduction | Structural joint changes may remain |
| Sleep quality and apnea | Moderate to good with full team approach | May need additional sleep medicine intervention |
| Dental concerns | Stabilization, improved orthodontic outcome | Existing structural changes do not reverse |
Adult tongue tie is real, it is common in the undiagnosed adult population, and it is treatable. If you recognize your own experience in what you have read here, the next step is seeking assessment from a qualified provider. The combination of a thorough diagnosis, a skilled release procedure, and committed myofunctional therapy gives adults the genuine opportunity to address a restriction that may have been quietly affecting their life in ways small and large for as long as they can remember.